
간세포암
 | |
|---|---|
| 다른 이름 | Hepatoma |
 | |
| C형 간염 양성인 환자의 간세포암종. 부검 표본. | |
| 진료과 | 종양학 |
간세포암(Hepatocellular carcinoma, HCC[1])은 성인에서 가장 흔한 원발성 간암 유형이며 현재 간경변증 환자의 가장 흔한 사망 원인이다.[2] 간세포암은 전 세계적으로 암 관련 사망의 세 번째 주요 원인이다.[3]
간세포암의 발병은 만성 간 손상 및 염증 환경에서 발생하는 섬유증과 간경변에 기인한다. 후자는 만성 바이러스성 간염 감염(B형 또는 C형 간염) 또는 알코올, 아플라톡신 또는 피롤리지딘 알칼로이드와[4] 같은 독소에 대한 노출과 밀접한 관련이 있다. 혈색소 침착증 및 알파 1-항트립신 결핍과 같은 특정 질병은 간세포암 발병 위험을 현저히 높인다. 대사 증후군과 비알코올성 지방간염도 간세포암의 위험 요인으로 점점 더 많이 인식되고 있다.[5]: 870–873
다른 암과 마찬가지로 간세포암의 치료와 예후는 종양 조직학, 크기, 암이 얼마나 퍼졌는지, 전반적인 건강 상태에 따라 달라진다.
간세포암 발병의 대부분과 치료 후 생존율이 가장 낮은 국가는 아시아와 사하라 사막 이남의 아프리카로, B형 간염 감염이 만연하고 출생 시 감염되는 경우가 많다. 미국과 기타 개발도상국에서는 C형 간염 바이러스 감염의 증가로 인해 간세포암 발생률이 증가하고 있다. 알 수 없는 이유로 남성에서 여성보다 3배 이상 흔하다.[5]: 870–873
징후 및 증상[편집]
대부분의 간세포암은 이미 만성 간질환의 징후와 증상이 있는 사람에게서 발생한다. 암 발견 당시에는 증상이 악화되거나 증상이 없을 수도 있다. 간세포암은 복통, 메스꺼움, 구토 또는 피로감과 같은 비특이적 증상을 나타낼 수 있다.[6] 간 질환과 더 밀접한 관련이 있는 증상으로는 황달이라고도 하는 노란 피부, 복강 내 체액으로 인한 복부 부종, 혈액 응고 이상으로 인한 쉽게 멍이 드는 증상, 식욕 부진, 의도하지 않은 체중 감소, 복통, 메스꺼움, 구토 또는 피로감 등이 있다.[6]
위험 요소[편집]
간세포암은 주로 간경변증 환자에게서 발생하므로 위험 요인에는 일반적으로 간경변증을 유발할 수 있는 만성 간 질환을 유발하는 요인이 포함된다. 하지만 특정 위험 요인은 다른 요인보다 간세포암종과 더 높은 연관성을 보인다. 예를 들어, 과음은 간경변의 60~70%를 유발하는 것으로 추정되지만, 간세포암의 대부분은 바이러스성 간염으로 인한 간경변에서 발생한다.[7] 알려진 위험 요인은 다음과 같다
- 만성 바이러스성 간염(전 세계 80% 사례의 원인으로 추정)
- 독소:
- 알코올 사용 장애: 간경변의 가장 흔한 원인[7]
- 아플라톡신
- 철분 과부하 상태(혈색소 침착증)
- 피롤리지딘 알칼로이드
- 대사:
- 선천성 장애:
이러한 위험 요인의 중요성은 전 세계적으로 다양하다. 중국 남동부와 같이 B형 간염 감염이 만연한 지역에서는 B형 간염이 주요 원인이다.[17] 미국과 같이 B형 간염 백신 접종으로 대부분 보호받는 인구에서 간세포암은 만성 C형 간염, 비만, 과도한 알코올 사용과 같은 간경변의 원인과 가장 많이 연관되어 있다.[18]
간세포 선종과 같은 특정 양성 간 종양은 때때로 공존하는 악성 간세포암과 연관될 수 있다. 양성 선종과 관련된 악성 종양의 실제 발생률에 대한 증거는 제한적이지만, 간 선종의 크기는 악성 종양의 위험과 일치하는 것으로 간주되므로 더 큰 종양은 수술로 제거할 수 있다. 선종의 특정 아형, 특히 베타 카테닌 활성화 돌연변이가 있는 선종은 특히 간세포암의 위험 증가와 관련이 있다.[18]
만성 간 질환은 어린이와 청소년에게 드물지만 선천성 간 질환은 간세포암종 발병 가능성을 높이는 것과 관련이 있다.[19] 특히 담도 폐쇄증, 영아 담즙 정체, 글리코겐 저장 질환 및 기타 간경변 질환이있는 소아는 어린 시절에 간세포 성 간암이 발생하기 쉽다.
희귀한 섬유라멜라 변종 간세포암에 걸린 젊은 성인에게는 간경변이나 간염과 같은 전형적인 위험 요인이 없을 수 있다.
당뇨병[편집]
제2형 당뇨병 환자의 간세포암종 위험은 당뇨병 유병 기간과 치료 프로토콜에 따라 비당뇨병 환자의 2.5배[11] ~ 7.1배[20]에 달한다.[21] 이러한 위험 증가의 원인으로 의심되는 것은 순환 인슐린 농도로, 인슐린 조절이 잘 되지 않거나 인슐린 분비량을 증가시키는 치료를 받는 당뇨병 환자는 순환 인슐린 농도를 낮추는 치료를 받는 당뇨병 환자보다 간세포암 위험이 훨씬 더 높다.[11][20][22][23] 반면, 인슐린 농도가 높아지지 않도록 인슐린을 엄격하게 조절하는 일부 당뇨병 환자는 일반인과 구별할 수 없을 정도로 낮은 위험 수치를 보인다.[20][22] 따라서 이러한 현상은 제2형 당뇨병에만 국한된 것이 아니며, 대사 증후군(특히 비알코올성 지방간 질환의 증거가 있는 경우)과 같은 다른 질환에서도 인슐린 조절 장애가 발견되고 이 경우에도 위험이 더 크다는 증거가 존재하기 때문이다.[24][25] 아나볼릭 스테로이드 남용자가 더 위험하다는 주장이 있지만(인슐린 및 IGF 악화로 인한 것으로 추정됨[26][27]), 확인된 유일한 증거는 아나볼릭 스테로이드 사용자가 양성 간세포 선종이 더 위험한 간세포 암종으로 변할 가능성이 더 높다는 것이다.[28][29]
병인[편집]
간세포암은 다른 암과 마찬가지로 후성유전학적 변화와 돌연변이가 세포 기계에 영향을 미쳐 세포가 더 빠른 속도로 복제되거나 세포가 세포 사멸을 피하게 될 때 발생한다.[30]
특히 B형 및 C형 간염의 만성 감염은 신체 자체의 면역 체계가 바이러스에 감염된 간세포를 반복적으로 공격하게 함으로써 간세포암의 발병을 도울 수 있다.[31] 활성화된 면역계 염증 세포는 활성 산소종과 산화질소 반응성 종과 같은 활성 산소를 방출하여 DNA 손상을 일으키고 발암성 유전자 돌연변이를 일으킬 수 있다.[32] 활성 산소종은 또한 DNA 복구 부위에서 후성유전학적 변화를 일으킨다.[33]
이러한 손상과 복구의 지속적인 주기는 복구 과정에서 실수로 이어져 발암으로 이어질 수 있지만, 현재로서는 이 가설이 만성 C형 간염에 더 적용 가능하다. 만성 C형 간염은 간경변 단계를 거쳐 간세포암을 유발한다. 그러나 만성 B형 간염에서는 바이러스 게놈이 감염된 세포에 통합되어 간경변증이 없는 간에서 간세포암이 직접적으로 발생할 수 있다. 또는 다량의 에탄올을 반복적으로 섭취하는 것도 비슷한 효과를 가져올 수 있다. 특정 아스페르길루스 진균의 독소인 아플라톡신은 발암 물질이며 간에 축적되어 간세포암의 발암을 돕는다. 중국과 서아프리카와 같은 환경에서 아플라톡신과 B형 간염의 높은 유병률로 인해 이 지역에서는 간세포암 발병률이 상대적으로 높다. A형 간염과 같은 다른 바이러스성 간염은 만성 감염이 될 가능성이 없으므로 간세포암과 관련이 없다.[18]
진단[편집]
간세포암 진단 방법은 의료 영상의 발전과 함께 발전해 왔다. 무증상 환자와 간 질환 증상이 있는 환자 모두 혈액 검사와 영상 평가를 통해 평가한다. 과거에는 간세포암 진단을 증명하기 위해 종양 생검이 필요했다. 그러나 영상(특히 MRI) 소견은 조직 병리학적 확인 없이도 충분히 결정적일 수 있다.[18]
건강검진[편집]
간세포암은 여전히 높은 사망률과 관련이 있는데, 이는 부분적으로는 초기 진단이 일반적으로 질병의 진행 단계에서 발생하기 때문이다. 다른 암과 마찬가지로 간세포암도 질병 진행 초기에 치료를 시작하면 예후가 크게 개선된다. 간세포암의 대부분은 특정 만성 간 질환, 특히 간경변증 환자에게서 발생하기 때문에 이러한 집단에서는 일반적으로 간 검진이 권장된다. 구체적인 검진 지침은 임상적 영향에 대한 증거가 나오면서 시간이 지남에 따라 계속 발전하고 있다. 미국에서 가장 일반적으로 준수되는 가이드라인은 미국 간질환 연구협회(AASLD)에서 발표한 가이드라인으로, 간경변증 환자에게 종양 표지자인 알파태아단백(AFP)의 혈중 농도 측정 여부와 관계없이 6개월마다 초음파 검사를 권장하고 있다.[34] AFP 수치가 높으면 간세포암종 활동과 관련이 있지만, 그 신뢰도는 일관성이 없을 수 있다. 수치가 20을 초과하면 민감도는 41-65%, 특이도는 80-94%이다. 그러나 수치가 200을 초과하면 민감도는 31, 특이도는 99%이다.[35]
초음파에서 간세포암은 종종 뚜렷하지 않은 경계와 거칠고 불규칙한 내부 에코를 가진 작은 저에코 병변으로 나타난다. 종양이 성장하면 섬유화, 지방 변화 및 석회화로 인해 이질적으로 보일 수 있다. 이러한 이질성은 간경변 및 주변 간 실질과 유사하게 보일 수 있다. 체계적 문헌고찰에 따르면 이식 또는 절제된 간을 참조 표준으로 한 병리학적 검사와 비교했을 때 민감도는 60%(95% CI 44-76%), 특이도는 97%(95% CI 95-98%)로 나타났다. AFP 상관관계가 있는 경우 민감도는 79%로 증가한다.[36]
가장 효과적인 선별 검사 프로토콜에 대한 논란은 여전히 남아 있다. 예를 들어, 일부 데이터는 B형 간염 감염자 선별 검사와 관련된 사망률 감소를 뒷받침하지만, AASLD는 "만성 C형 간염 또는 지방간 질환에 이차적으로 간경변증이 있는 서양인 인구에 대한 무작위 임상시험이 없기 때문에 이러한 간경변증 환자 집단에서 선별 검사가 실제로 사망률 감소로 이어지는지에 대해서는 논란이 있다."라고 지적한다.[34]
고위험군[편집]
간세포암이 의심되는 사람(예: 알파태아단백 및 데감마카복시프로트롬빈 수치)의 경우, 증상이 있거나 혈액 검사에서 비정상적인 수치가 있는 경우 평가 시 CT 또는 MRI 스캔으로 간 영상을 촬영해야 한다. 이러한 스캔은 해석하는 방사선 전문의가 간 병변을 더 잘 감지하고 정확하게 분류할 수 있도록 간 관류의 여러 단계에서 정맥 조영제를 사용하여 수행하는 것이 최선이다. 간세포암 종양의 특징적인 혈류 패턴으로 인해, 검출된 간 병변의 특정 관류 패턴이 간세포암 종양을 결정적으로 검출할 수 있다. 또는 스캔에서 불확실한 병변을 감지하고 병변의 물리적 샘플을 확보하여 추가 평가를 수행 할 수 있다..[18][37]
이미징[편집]

간세포 암종에 대한 간을 평가하기 위해 초음파, CT 스캔 및 MRI를 사용할 수 있다. CT와 MRI에서 간세포암은 세 가지 뚜렷한 성장 패턴을 보일 수 있다
- 하나의 큰 종양
- 다발성 종양
- 침윤성 성장 패턴을 가진 잘 정의되지 않은 종양
CT 진단에 대한 체계적 문헌고찰에 따르면 간을 적출하거나 절제한 간을 참조 표준으로 한 병리 검사와 비교했을 때 민감도는 68%(95% CI 55-80%), 특이도는 93%(95% CI 89-96%)로 나타났다. 삼상 나선형 CT의 경우 민감도는 90% 이상이었지만 부검 연구에서는 이러한 데이터가 확인되지 않았다.[36]
그러나 MRI는 전리방사선 없이 간을 고해상도 이미지로 촬영할 수 있다는 장점이 있다. 간세포암은 T2 강조 영상에서는 고강도 패턴으로, T1 강조 영상에서는 저강도 패턴으로 나타난다. MRI의 장점은 간세포암과 재생 결절을 구별하기 어려운 간경변 환자에서 초음파 및 CT에 비해 민감도와 특이도가 향상되었다는 점이다. 체계적 문헌고찰에 따르면 간을 적출하거나 절제한 간을 참조 표준으로 한 병리학적 검사와 비교했을 때 민감도는 81%(95% CI 70-91%), 특이도는 85%(95% CI 77-93%)로 나타났다.[36] 가돌리늄 조영 증강 영상과 확산 가중 영상을 결합하면 민감도가 더욱 높아진다.
MRI는 CT보다 더 민감하고 특이적이다.[38]
간 영상 보고 및 데이터 시스템(LI-RADS)은 CT 및 MRI에서 발견된 간 병변을 보고하기 위한 분류 시스템이다. 영상의학과 전문의는 이 표준화된 시스템을 사용하여 의심스러운 병변을 보고하고 악성 가능성을 추정한다. 카테고리는 암에 대한 우려 순서대로 LI-RADS (LR) 1에서 5까지이다.[39] 특정 영상 기준이 충족되는 경우 간세포암 진단을 확인하기 위해 조직검사를 할 필요는 없다.[18]
병리학[편집]

Macroscopically, liver cancer appears as a nodular or infiltrative tumor. The nodular type may be solitary (large mass) or multiple (when developed as a complication of cirrhosis). Tumor nodules are round to oval, gray or green (if the tumor produces bile), well circumscribed but not encapsulated. The diffuse type is poorly circumscribed and infiltrates the portal veins, or the hepatic veins (rarely).[18]
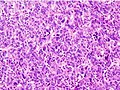
Microscopically, the four architectural and cytological types (patterns) of hepatocellular carcinoma are: fibrolamellar, pseudoglandular (adenoid), pleomorphic (giant cell), and clear cell. In well-differentiated forms, tumor cells resemble hepatocytes, form trabeculae, cords, and nests, and may contain bile pigment in the cytoplasm. In poorly differentiated forms, malignant epithelial cells are discohesive, pleomorphic, anaplastic, and giant. The tumor has a scant stroma and central necrosis because of the poor vascularization.[40] A fifth form – lymphoepithelioma like hepatocellular carcinoma – has also been described.
거시적으로 간암은 결절성 또는 침윤성 종양으로 나타난다. 결절형은 단일(큰 덩어리) 또는 다발성(간경변의 합병증으로 발생하는 경우)일 수 있다. 종양 결절은 원형에서 타원형, 회색 또는 녹색(종양이 담즙을 생성하는 경우)이며, 외피는 잘 둘러싸여 있지만 캡슐화되어 있지는 않다. 미만성 유형은 외곽이 잘 둘러싸여 있지 않고 문맥 또는 간정맥에 침투한다 (드물게).
현미경으로 볼 때 간세포암의 네 가지 구조적 및 세포학적 유형(패턴)은 섬유라멜라형, 선상(아데노이드), 다형성(거대세포), 투명세포이다. 잘 분화된 형태의 종양 세포는 간세포와 유사하며 섬유질, 끈, 둥지를 형성하고 세포질에 담즙 색소를 포함할 수 있다. 잘 분화되지 않은 형태의 악성 상피 세포는 원반형, 다형성, 역형성, 거대 세포이다. 종양은 혈관이 잘 형성되지 않아 기질이 부족하고 중심이 괴사한다. 간세포암과 같은 다섯 번째 형태인 림프상피종도 설명되어 있다.[41][42]
-
 잘 분화된 간세포암종
잘 분화된 간세포암종 -
 중간 정도의 분화 간세포암.
중간 정도의 분화 간세포암. -
 제대로 분화되지 않은 간세포암
제대로 분화되지 않은 간세포암



병기[편집]
BCLC 스테이징 시스템
간세포암의 예후는 종양의 병기와 간경변의 영향으로 인한 간 기능에 의해 영향을 받는다.[43]
간세포암의 병기 분류는 여러 가지가 있다. 그러나 간세포암종 분류에 영향을 미치는 모든 특징을 완전히 포괄하는 암종의 고유한 특성으로 인해 분류 시스템에는 종양의 크기와 수, 혈관 침범 및 간외 전이 유무, 간 기능(혈청 빌리루빈 및 알부민 수치, 복수 유무, 문맥 고혈압), 환자의 전반적인 건강 상태(ECOG 분류 및 증상 유무에 따라 정의됨)가 포함되어야 한다.[43]
사용 가능한 모든 병기 분류 시스템 중에서 바르셀로나 클리닉 간암 병기 분류는 위의 모든 특성을 포괄한다. 이 병기 분류는 치료 대상자를 선택하는 데 사용할 수 있다.[44]
| 병기 | 설명 | Child-Pugh 분류 | ECOG performance status |
|---|---|---|---|
| 0(초기 단계) | 단일 결절, 3cm 미만 | A | 0 |
| A(초기 단계) | 1-3 결절, 모두 3cm 미만 | A or B | |
| B(중간 단계) | 다발성 결절성 종양 | ||
| C(고급 단계) | 문맥 침범 및 간외 확산 | 1 or 2 | |
| D(최종 단계) | 심각한 간 손상 | C | 3 or 4 |
치료의 가이드라인으로 사용되는 중요한 특징은 다음과 같다.
- 크기
- 스프레드(병기)
- 간 혈관의 침범
- 종양 캡슐의 존재
- 간외 전이의 존재
- 딸 결절의 존재
- 종양의 혈관생성
MRI는 종양 캡슐의 존재를 감지하는 데 가장 적합한 영상 촬영 방법이다.
가장 흔한 전이 부위는 폐, 복부 림프절, 뼈이다.[48]
예방[편집]
B형 및 C형 간염은 간세포암의 주요 원인 중 하나이므로 간세포암을 예방하기 위해서는 감염을 예방하는 것이 중요하다. 따라서 어린 시절 B형 간염 예방 접종을 받으면 향후 간암 위험을 줄일 수 있다.[49] 간경변 환자의 경우 알코올 섭취를 피해야한다. 또한 일부 환자에게는 혈색소 침착증 선별 검사가 도움이 될 수 있다.[50] 만성 간 질환이있는 사람들에게 간세포 암종 선별 검사가 결과를 개선하는지 여부는 불분명하다.[51]
각주[편집]
- ↑ Shetty S, Sharma N, Ghosh K (March 2016). “Epidemiology of hepatocellular carcinoma (HCC) in hemophilia”. 《Critical Reviews in Oncology/Hematology》 99: 129–133. doi:10.1016/j.critrevonc.2015.12.009. PMID 26754251.
- ↑ Forner A, Llovet JM, Bruix J (March 2012). “Hepatocellular carcinoma”. 《Lancet》 379 (9822): 1245–1255. doi:10.1016/S0140-6736(11)61347-0. PMID 22353262. S2CID 24927898.
- ↑ “Global Cancer Observatory”. 《gco.iarc.fr》. 2021년 6월 24일에 확인함.
- ↑ Tan DJ, Wong C, Ng CH, Poh CW, Jain SR, Huang DQ, Muthiah MD (January 2021). “A Meta-Analysis on the Rate of Hepatocellular Carcinoma Recurrence after Liver Transplant and Associations to Etiology, Alpha-Fetoprotein, Income and Ethnicity”. 《Journal of Clinical Medicine》 10 (2): 238. doi:10.3390/jcm10020238. PMC 7828059. PMID 33440759.
- ↑ 가 나 Kumar V, Fausto N, Abbas A, 편집. (2015). 《Robbins & Cotran Pathologic Basis of Disease》 9판. Saunders. ISBN 978-1-4557-2613-4.
- ↑ 가 나 “Liver cancer overview”. Mayo Clinic.
- ↑ 가 나 Heidelbaugh JJ, Bruderly M (September 2006). “Cirrhosis and chronic liver failure: part I. Diagnosis and evaluation”. 《American Family Physician》 74 (5): 756–762. PMID 16970019.
- ↑ Alter MJ (May 2007). “Epidemiology of hepatitis C virus infection”. 《World Journal of Gastroenterology》 13 (17): 2436–2441. doi:10.3748/wjg.v13.i17.2436. PMC 4146761. PMID 17552026.
- ↑ White DL, Kanwal F, El-Serag HB (December 2012). “Association between nonalcoholic fatty liver disease and risk for hepatocellular cancer, based on systematic review”. 《Clinical Gastroenterology and Hepatology》 10 (12): 1342–1359.e2. doi:10.1016/j.cgh.2012.10.001. PMC 3501546. PMID 23041539.
- ↑ “NAFLD vs. NASH”. 《Medicine Specifics》 (미국 영어). 2019년 11월 11일. 2021년 6월 22일에 확인함.
- ↑ 가 나 다 El-Serag HB, Hampel H, Javadi F (March 2006). “The association between diabetes and hepatocellular carcinoma: a systematic review of epidemiologic evidence”. 《Clinical Gastroenterology and Hepatology》 4 (3): 369–380. doi:10.1016/j.cgh.2005.12.007. PMID 16527702.
Diabetes is associated with an increased risk for HCC. However, more research is required to examine issues related to the duration and treatment of diabetes, and confounding by diet and obesity
- ↑ Wang XW, Hussain SP, Huo TI, Wu CG, Forgues M, Hofseth LJ, 외. (December 2002). “Molecular pathogenesis of human hepatocellular carcinoma”. 《Toxicology》. 181-182: 43–47. doi:10.1016/S0300-483X(02)00253-6. PMID 12505283.
Recent studies in our laboratory have identified several potential factors that may contribute to the pathogenesis of HCC...For example, oxyradical overload diseases such as Wilson disease and hemochromatosis result in the generation of oxygen/nitrogen species that can cause mutations in the p53 tumour suppressor gene
- ↑ Cheng WS, Govindarajan S, Redeker AG (February 1992). “Hepatocellular carcinoma in a case of Wilson's disease”. 《Liver》 12 (1): 42–45. doi:10.1111/j.1600-0676.1992.tb00553.x. PMID 1314321.
The patient described here was the oldest and only the third female patient with hepatocellular carcinoma complicating Wilson's disease to be reported in the literature
- ↑ Wilkinson ML, Portmann B, Williams R (August 1983). “Wilson's disease and hepatocellular carcinoma: possible protective role of copper”. 《Gut》 24 (8): 767–771. doi:10.1136/gut.24.8.767. PMC 1420230. PMID 6307837.
As copper has been shown to protect against chemically induced hepatocellular carcinoma in rats, this may be the reason for the extreme rarity of hepatocellular carcinoma in patients with Wilson's disease and possibly in other liver diseases with hepatic copper overload
- ↑ Huang YC, Tsan YT, Chan WC, Wang JD, Chu WM, Fu YC, 외. (April 2015). “Incidence and survival of cancers among 1,054 hemophilia patients: A nationwide and 14-year cohort study”. 《American Journal of Hematology》 90 (4): E55–E59. doi:10.1002/ajh.23947. PMID 25639564.
- ↑ Shetty S, Sharma N, Ghosh K (March 2016). “Epidemiology of hepatocellular carcinoma (HCC) in hemophilia”. 《Critical Reviews in Oncology/Hematology》 99: 129–133. doi:10.1016/j.critrevonc.2015.12.009. PMID 26754251.
- ↑ Tanaka M, Katayama F, Kato H, Tanaka H, Wang J, Qiao YL, Inoue M (2011). “Hepatitis B and C virus infection and hepatocellular carcinoma in China: a review of epidemiology and control measures”. 《Journal of Epidemiology》 21 (6): 401–416. doi:10.2188/jea.JE20100190. PMC 3899457. PMID 22041528.
- ↑ 가 나 다 라 마 바 사 Balogh J, Victor D, Asham EH, Burroughs SG, Boktour M, Saharia A, 외. (2016). “Hepatocellular carcinoma: a review”. 《Journal of Hepatocellular Carcinoma》 3: 41–53. doi:10.2147/JHC.S61146. PMC 5063561. PMID 27785449.
- ↑ Mehta P (2019년 11월 10일). Windle ML, Bergstrom SK, 편집. “Pathophysiology”. 《Emedicine》. MedScape. 2010년 5월 12일에 확인함.
- ↑ 가 나 다 Hassan MM, Curley SA, Li D, Kaseb A, Davila M, Abdalla EK, 외. (April 2010). “Association of diabetes duration and diabetes treatment with the risk of hepatocellular carcinoma”. 《Cancer》 116 (8): 1938–1946. doi:10.1002/cncr.24982. PMC 4123320. PMID 20166205.
Diabetes appears to increase the risk of HCC, and such risk is correlated with a long duration of diabetes. Relying on dietary control and treatment with sulfonylureas or insulin were found to confer the highest magnitude of HCC risk, whereas treatment with biguanides or thiazolidinediones was associated with a 70% HCC risk reduction among diabetics.
- ↑ Charitha, Gorantla Sri; Chaitanya, Nyshadham S. N.; Reddy, Aramati Bindu Madhava (2022년 1월 1일), Nagaraju, Ganji Purnachandra; Vadde, Ramakrishna, 편집., “Chapter 22 - LKB1/STK11-mediated signal transduction in hepatocellular carcinoma”, 《Theranostics and Precision Medicine for the Management of Hepatocellular Carcinoma, Volume 2》 (영어) (Academic Press), 357–367쪽, doi:10.1016/b978-0-323-98807-0.00017-x, ISBN 978-0-323-98807-0, 2023년 4월 6일에 확인함
- ↑ 가 나 Donadon V, Balbi M, Ghersetti M, Grazioli S, Perciaccante A, Della Valentina G, 외. (May 2009). “Antidiabetic therapy and increased risk of hepatocellular carcinoma in chronic liver disease”. 《World Journal of Gastroenterology》 15 (20): 2506–2511. doi:10.3748/wjg.15.2506. PMC 2686909. PMID 19469001.
Our study confirms that type 2 diabetes mellitus is an independent risk factor for HCC and pre-exists in the majority of HCC patients. Moreover, in male patients with type 2 diabetes mellitus, our data shows a direct association of HCC with insulin and sulphanylureas treatment and an inverse relationship with metformin therapy.
- ↑ Donadon V, Balbi M, Ghersetti M, Grazioli S, Perciaccante A, Della Valentina G, 외. (May 2009). “Antidiabetic therapy and increased risk of hepatocellular carcinoma in chronic liver disease”. 《World Journal of Gastroenterology》 15 (20): 2506–2511. doi:10.3748/wjg.15.2506. PMC 2686909. PMID 19469001.
- ↑ Siegel AB, Zhu AX (December 2009). “Metabolic syndrome and hepatocellular carcinoma: two growing epidemics with a potential link”. 《Cancer》 115 (24): 5651–5661. doi:10.1002/cncr.24687. PMC 3397779. PMID 19834957.
The majority of 'cryptogenic' HCC in the United States is attributed to nonalcoholic fatty liver disease (NAFLD), a hepatic manifestation of the metabolic syndrome... It is predicted that metabolic syndrome will lead to large increases in the incidence of HCC over the next decades. A better understanding of the relation between these two diseases ultimately should lead to improved screening and treatment options for patients with HCC.
- ↑ Stickel F, Hellerbrand C (October 2010). “Non-alcoholic fatty liver disease as a risk factor for hepatocellular carcinoma: mechanisms and implications”. 《Gut》 59 (10): 1303–1307. doi:10.1136/gut.2009.199661. PMID 20650925. S2CID 31016985.
Based on the known association of NAFLD with IR and MS, approximately two-thirds of the patients were obese and/or diabetic, 4 and a remarkable 25% of these patients had no cirrhosis... Therefore, it is particularly worrying that the most persuasive evidence for an association between NAFLD and HCC derives from studies on the risk of HCC in patients with metabolic syndrome
- ↑ Höpfner M, Huether A, Sutter AP, Baradari V, Schuppan D, Scherübl H (May 2006). “Blockade of IGF-1 receptor tyrosine kinase has antineoplastic effects in hepatocellular carcinoma cells”. 《Biochemical Pharmacology》 71 (10): 1435–1448. doi:10.1016/j.bcp.2006.02.006. PMID 16530734.
Inhibition of IGF-1R tyrosine kinase (IGF-1R-TK) by NVP-AEW541 induces growth inhibition, apoptosis and cell cycle arrest in human HCC cell lines without accompanying cytotoxicity. Thus, IGF-1R-TK inhibition may be a promising novel treatment approach in HCC.
- ↑ Huynh H, Chow PK, Ooi LL, Soo KC (March 2002). “A possible role for insulin-like growth factor-binding protein-3 autocrine/paracrine loops in controlling hepatocellular carcinoma cell proliferation”. 《Cell Growth & Differentiation》 13 (3): 115–122. PMID 11959812. 2021년 4월 15일에 원본 문서에서 보존된 문서. 2023년 10월 27일에 확인함.
Our data indicate that loss of autocrine/paracrine IGFBP-3 loops may lead to HCC tumor growth and suggest that modulating production of the IGFs, IGFBP-3, and IGF-IR may represent a novel approach in the treatment of HCC.
- ↑ Martin NM, Abu Dayyeh BK, Chung RT (July 2008). “Anabolic steroid abuse causing recurrent hepatic adenomas and hemorrhage”. 《World Journal of Gastroenterology》 14 (28): 4573–4575. doi:10.3748/wjg.14.4573. PMC 2731289. PMID 18680242.
This is the first reported case of hepatic adenoma re-growth with recidivistic steroid abuse, complicated by life-threatening hemorrhage.
- ↑ Gorayski P, Thompson CH, Subhash HS, Thomas AC (January 2008). “Hepatocellular carcinoma associated with recreational anabolic steroid use”. 《British Journal of Sports Medicine》 42 (1): 74–5; discussion 75. doi:10.1136/bjsm.2007.03932. PMID 18178686. S2CID 21900098.
Malignant transformation to HCC from a pre-existing hepatic adenoma confirmed by immunohistochemical study has previously not been reported in athletes taking anabolic steroids. Further studies using screening programmes to identify high-risk individuals are recommended.
- ↑ Shibata T, Aburatani H (June 2014). “Exploration of liver cancer genomes”. 《Nature Reviews. Gastroenterology & Hepatology》 11 (6): 340–349. doi:10.1038/nrgastro.2014.6. PMID 24473361. S2CID 8611393.
- ↑ Chen CJ, Yang HI, Su J, Jen CL, You SL, Lu SN, 외. (January 2006). “Risk of hepatocellular carcinoma across a biological gradient of serum hepatitis B virus DNA level”. 《JAMA》 295 (1): 65–73. doi:10.1001/jama.295.1.65. PMID 16391218.
- ↑ Yang SF, Chang CW, Wei RJ, Shiue YL, Wang SN, Yeh YT (2014). “Involvement of DNA damage response pathways in hepatocellular carcinoma”. 《BioMed Research International》 2014: 153867. doi:10.1155/2014/153867. PMC 4022277. PMID 24877058.
- ↑ Nishida N, Kudo M (2013). “Oxidative stress and epigenetic instability in human hepatocarcinogenesis”. 《Digestive Diseases》 31 (5–6): 447–453. doi:10.1159/000355243. PMID 24281019.
- ↑ 가 나 Heimbach JK, Kulik LM, Finn RS, Sirlin CB, Abecassis MM, Roberts LR, 외. (January 2018). “AASLD guidelines for the treatment of hepatocellular carcinoma”. 《Hepatology》 67 (1): 358–380. doi:10.1002/hep.29086. PMID 28130846.
- ↑ “Clinical features and diagnosis of primary hepatocellular carcinoma”. UptoDate. 2014년 2월 4일에 확인함.
- ↑ 가 나 다 Colli A, Fraquelli M, Casazza G, Massironi S, Colucci A, Conte D, Duca P (March 2006). “Accuracy of ultrasonography, spiral CT, magnetic resonance, and alpha-fetoprotein in diagnosing hepatocellular carcinoma: a systematic review”. 《The American Journal of Gastroenterology》 101 (3): 513–523. doi:10.1111/j.1572-0241.2006.00467.x. PMID 16542288. S2CID 9563077.
- ↑ “Benign Liver Tumors”. 《The Lecturio Medical Concept Library》. 2021년 7월 4일에 확인함.
- ↑ El-Serag HB, Marrero JA, Rudolph L, Reddy KR (May 2008). “Diagnosis and treatment of hepatocellular carcinoma”. 《Gastroenterology》 134 (6): 1752–1763. doi:10.1053/j.gastro.2008.02.090. PMID 18471552. S2CID 10418520.
- ↑ “Li-Rads”. 2017년 7월 11일에 원본 문서에서 보존된 문서. 2014년 2월 4일에 확인함.
- ↑ Hepatocellular carcinoma (Photo) 보관됨 2021-11-01 - 웨이백 머신 ATLAS OF PATHOLOGY
- ↑ Chan AW, Zhang Z, Chong CC, Tin EK, Chow C, Wong N (October 2019). “Genomic landscape of lymphoepithelioma-like hepatocellular carcinoma”. 《The Journal of Pathology》 249 (2): 166–172. doi:10.1002/path.5313. PMID 31168847. S2CID 174815950.
- ↑ Chan AW, Tong JH, Pan Y, Chan SL, Wong GL, Wong VW, 외. (March 2015). “Lymphoepithelioma-like hepatocellular carcinoma: an uncommon variant of hepatocellular carcinoma with favorable outcome”. 《The American Journal of Surgical Pathology》 39 (3): 304–312. doi:10.1097/pas.0000000000000376. PMID 25675010. S2CID 40384842.
- ↑ 가 나 Duseja A (August 2014). “Staging of hepatocellular carcinoma”. 《Journal of Clinical and Experimental Hepatology》 4 (Suppl 3): S74–S79. doi:10.1016/j.jceh.2014.03.045. PMC 4284240. PMID 25755615.
- ↑ Llovet JM, Brú C, Bruix J (1999). “Prognosis of hepatocellular carcinoma: the BCLC staging classification”. 《Seminars in Liver Disease》 19 (3): 329–338. doi:10.1055/s-2007-1007122. PMID 10518312. S2CID 23889399.
- ↑ “BCLC staging system and the Child-Pugh system ;Liver cancer ; Cancer Research UK”. 《www.cancerresearchuk.org》.
- ↑ “What is the Barcelona Clinic Liver Cancer (BCLC) system for hepatocellular carcinoma (HCC) staging?”. 《www.medscape.com》.
- ↑ Kinoshita A, Onoda H, Fushiya N, Koike K, Nishino H, Tajiri H (March 2015). “Staging systems for hepatocellular carcinoma: Current status and future perspectives”. 《World Journal of Hepatology》 7 (3): 406–424. doi:10.4254/wjh.v7.i3.406. PMC 4381166. PMID 25848467.
- ↑ Katyal S, Oliver JH, Peterson MS, Ferris JV, Carr BS, Baron RL (September 2000). “Extrahepatic metastases of hepatocellular carcinoma”. 《Radiology》 216 (3): 698–703. doi:10.1148/radiology.216.3.r00se24698. PMID 10966697.
- ↑ “Hepatitis B: Prevention and treatment”. 2013년 7월 24일에 원본 문서에서 보존된 문서. 2013년 8월 28일에 확인함. "WHO aims at controlling HBV worldwide to decrease the incidence of HBV-related chronic liver disease, cirrhosis, and hepatocellular carcinoma. by integrating HB vaccination into routine infant (and possibly adolescent) immunization programs."
- ↑ “Prevention”. 2010년 5월 12일에 확인함.
- ↑ Kansagara D, Papak J, Pasha AS, O'Neil M, Freeman M, Relevo R, 외. (August 2014). “Screening for hepatocellular carcinoma in chronic liver disease: a systematic review”. 《Annals of Internal Medicine》 161 (4): 261–269. doi:10.7326/M14-0558. PMID 24934699.